Scoliosis Treatment Without Surgery / Correcting Scoliosis
Scoliosis is a curve of the spine which affects approximately 3 out of every 100 people in the United States. Although scoliosis occurs in the spine, it can impact other areas of the body causing asymmetries and imbalances including…
One eye tilted higher than the other
- One shoulder higher than the other
- One shoulder blade sticks out more than the other
- One hip higher or more pronounced than the other
- One side of the rib cage higher than the other
- Body tilts to one side
- One leg appears shorter than the other
- Ribs stick out when full forward bend
Managing Scoliosis
While scoliosis may develop in babies (infantile idiopathic scoliosis), typical onset occurs in early teens (adolescent idiopathic scoliosis). As the word idiopathic suggests, there is no known cause for infantile or adolescent scoliosis. The earlier the scoliosis is identified and treated, the better the outcome of treatment. For all scoliosis treatments, the goal is to control or even reverse the curve and decrease the negative effects of the curve.
The two world wide organizations leading the research in scoliosis are:
1. The Society on Scoliosis Orthop[aedic and Rehabilitation Treatment (SOSORT)
2. Scoliosis Research Society (SRS)
SOSORT 2016 guidelines for scoliosis treatment consider several factors including:
- Bone age
- Degree of curvature
- Amount of rotation
Common approaches to managing Scoliosis include:
- Observation
- Physical Therapy Scoliosis Specific Exercises (PSSE)
- Night Bracing
- Soft Bracing
- Part Time Rigid Bracing (8-12 hours)
- Full-time Rigid Bracing (20-24 hours)
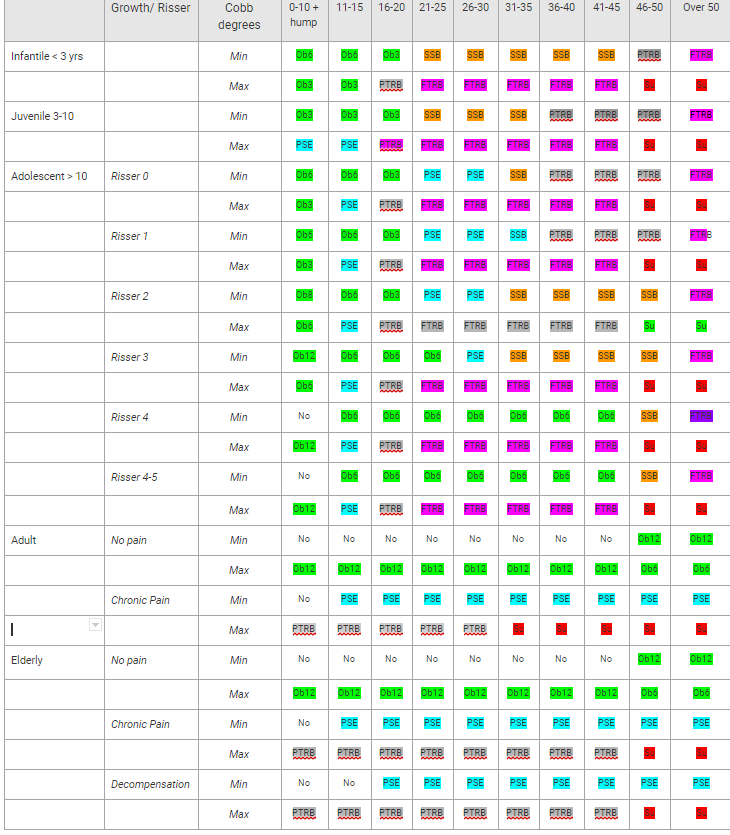
In 2011 SOSORT published guidelines for managing scoliosis. These guidelines are displayed in the charts below.
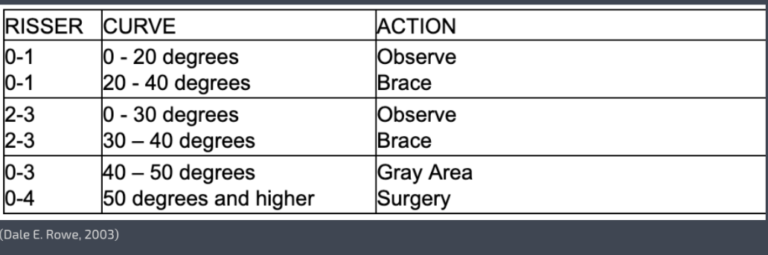
The SRS also has recommendation for adolescent scoliosis bracing:
Bracing
In this paragraph, we are going to discuss bracing benefits. Most importantly, it is important to realize that scoliosis curves tend to increase during rapid growth. For this reason, external support via a brace is recommended during adolescent growth years. The brace, worn full time or part time, tends to halt or reduce the curve progression. As a result, there are a variety of rigid braces (e.g., Milwaukee, Rigo, Cheneau, Boston, and others). Similarly, there are a handful of soft braces, however, these soft braces are less documented in the research. Current research does not indicate that any one brace is better than another, however it does indicate that full time brace wearing (20+ hours per day) correlates with the most favorable outcome. Bracing can be used for both adolescents and adults. With the adult brace the goal is to support the spine, unload deforming forces, reduce pain, and slow progression of the curve.
The Schroth Method
The Schroth Method is a nonsurgical option for scoliosis treatment. Katrina Schroth developed her three dimensional approach about 90 years ago with the aim of halting or reducing progression of her own scoliosis. Her therapy sought to reduce postural rotation, enhance mobility and stability, counter pain, and strengthen heart and lung function which all have long lasting effects.
Today, the Schroth Method is the standard for scoliosis therapy throughout the United States and Europe. All Schroth therapists are licensed physical therapists with additional training on the postural specific exercises. The method uses 3 dimensional exercises along with breathing to derotate the spine and reduce the curve.
Find a Schroth Therapist in your area.
Schroth Method Research
Certainly, the Schroth Method is successful,however, don’t simply take our word for it. Do your own research! Here are 5 randomized controlled studies (the most credible research) which support the Schroth Method for treating scoliosis. These include:
Some Helpful Links on the Net
Align Clinic
American Association of Neurological Surgeons (AANS). Scoliosis.
How the Schroth Method Works
National Scoliosis Foundation
Scoliosis Conservative Treatment: A review of literature
Scoliosis in Children and Adolescents
The Society on Scoliosis Orthop[aedic and Rehabilitation Treatment (SOSORT)
Scoliosis Research Society. (SRS)